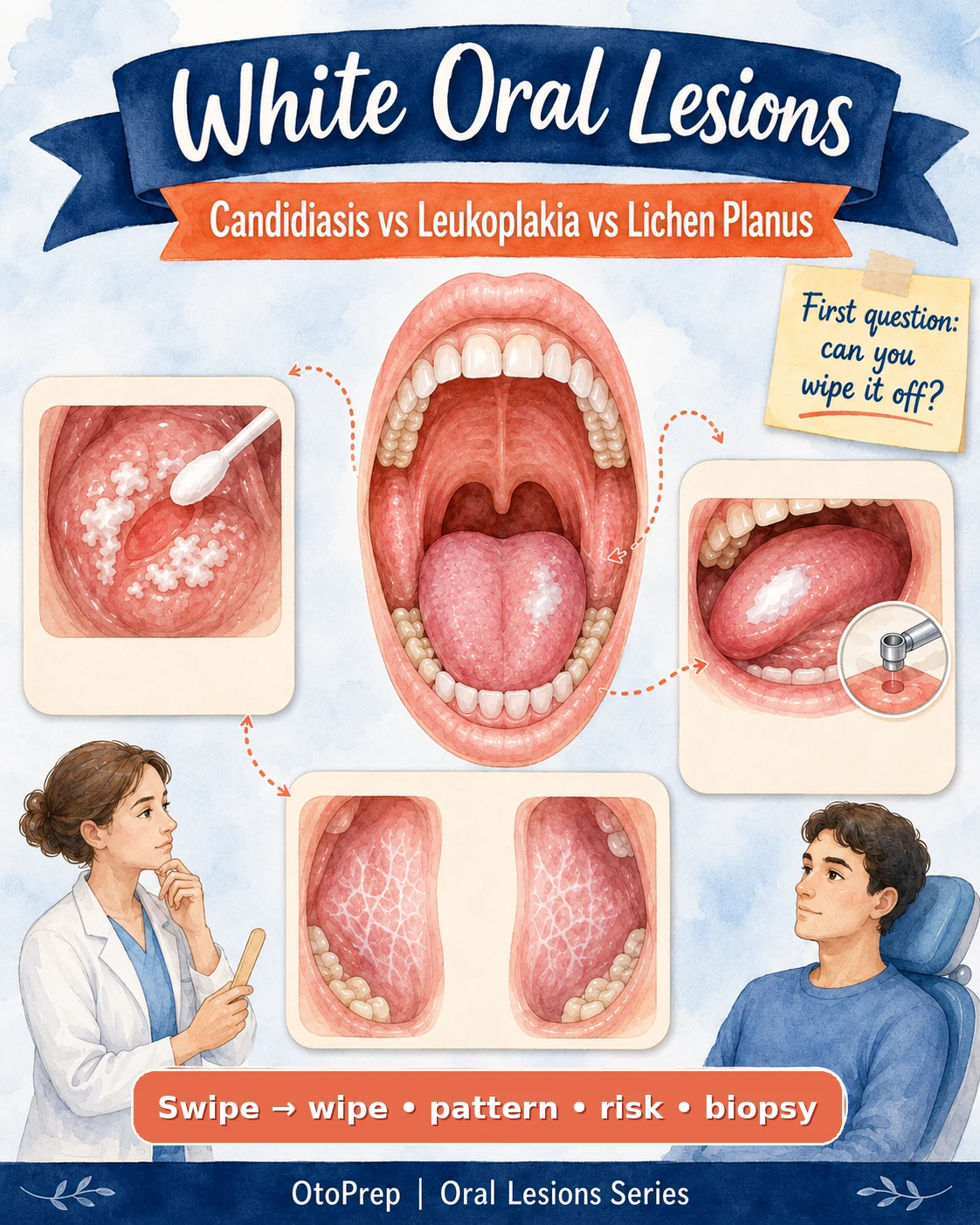
White Oral Lesions: the wipe test algorithm for ENT boards.
A white plaque in the mouth is not a diagnosis. The high-yield approach is to wipe it, pattern it, assess risk, treat what is treatable, and biopsy or refer what persists.
Exam line: “White plaque + no diagnosis = don’t just reassure.”
The 60-second overview: how to pattern white oral lesions
For board questions, do not start by memorising every possible white lesion. Start with the algorithm.
- Can it be wiped off? If yes, think pseudomembranous candidiasis first.
- Where is it? Buccal mucosa, lateral tongue and floor of mouth carry different implications.
- Is it symmetric? Bilateral lacy lesions favour classic oral lichen planus.
- Is there red, ulcerated or indurated change? Lower your biopsy/referral threshold.
- Did it respond to appropriate treatment? Treat the treatable, but review the response.
treat the treatable → review → biopsy or refer the persistent.

Step 1: the wipe test
The first practical question in a white oral lesion stem is simple: does the plaque wipe off?
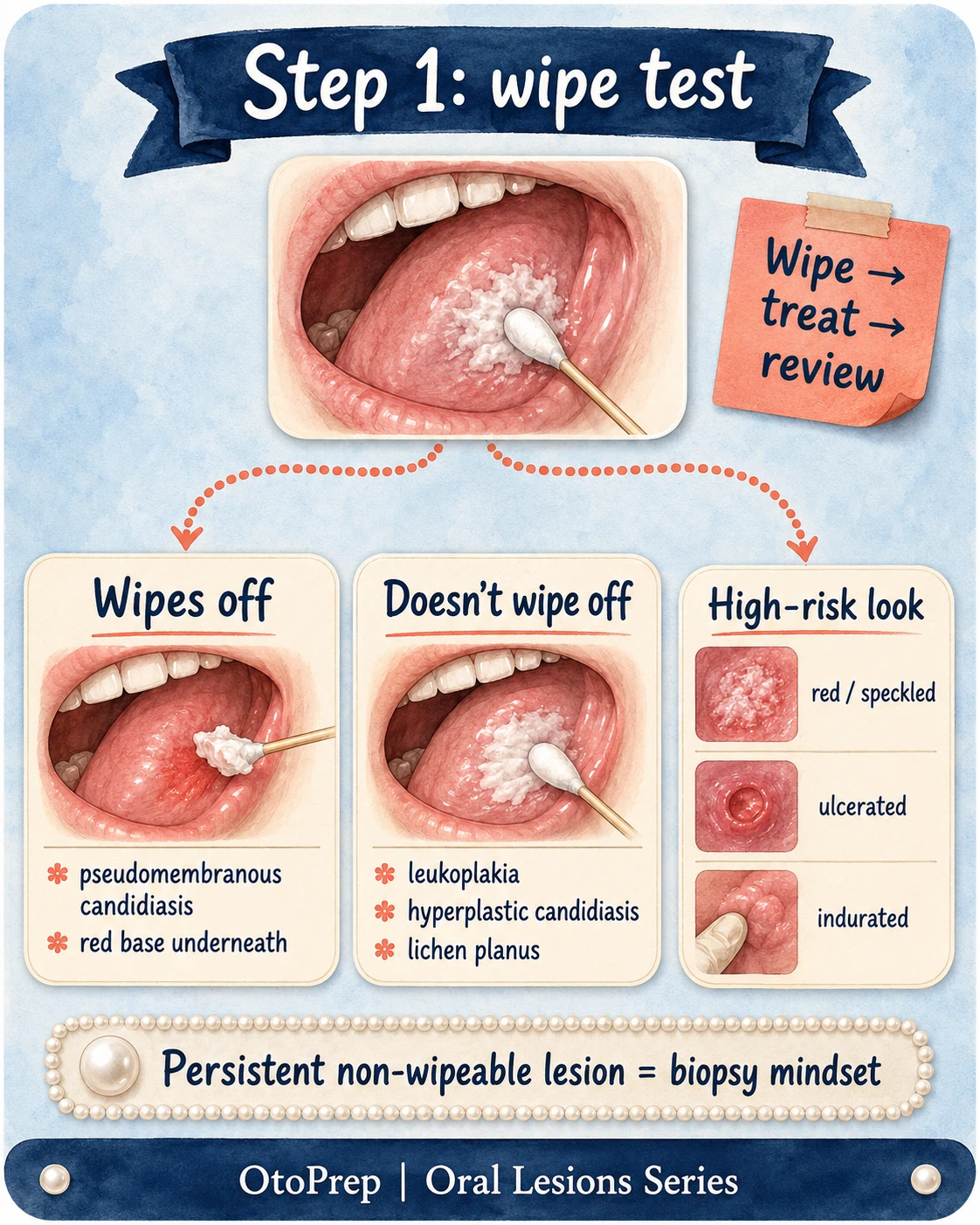
| Wipe test result | Most important board interpretation | Next step mindset |
|---|---|---|
| Wipes off | Pseudomembranous candidiasis rises to the top. | Treat candidiasis, address risk factors, then review. |
| Doesn’t wipe off | Do not automatically call it leukoplakia. | Pattern the lesion: lichen planus, frictional keratosis, hyperplastic candidiasis, dysplasia and leukoplakia are all in play. |
| Red, speckled, ulcerated or indurated | Higher-risk morphology. | Biopsy/referral threshold should be low. |
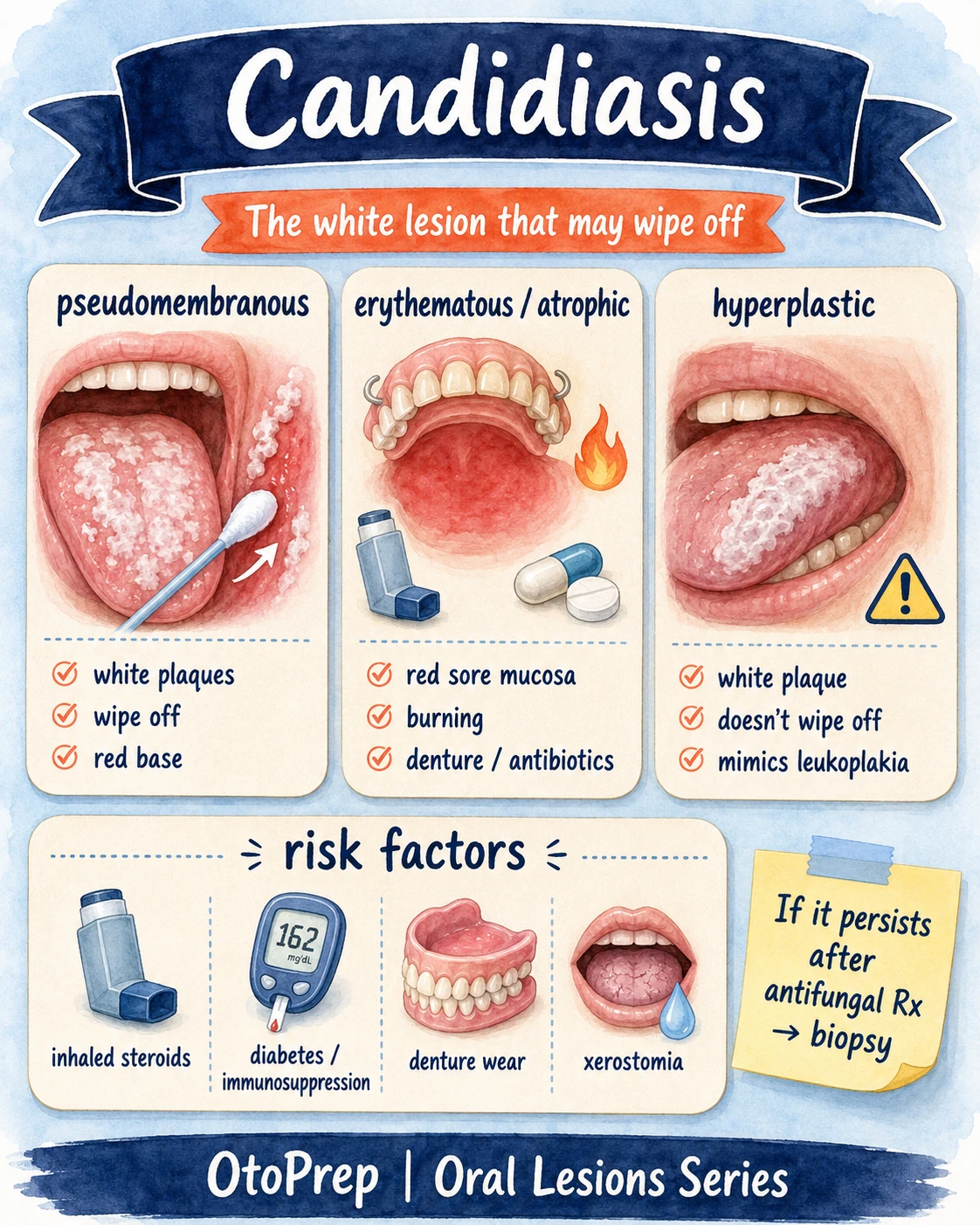
Oral candidiasis: the white lesion that may wipe off
Pseudomembranous candidiasis is the classic “white plaques that scrape away” diagnosis — but candidiasis is not always white and not always wipeable.
Pseudomembranous
- White plaques
- Usually wipe off
- Often leaves an erythematous base
Erythematous / atrophic
- Red sore mucosa
- Burning symptoms
- Often linked with dentures or antibiotics
Hyperplastic
- White plaque
- May not wipe off
- Can mimic leukoplakia
- Inhaled or topical corticosteroids
- Recent antibiotics
- Denture wear or poor denture hygiene
- Diabetes or immunosuppression
- Xerostomia or reduced salivary flow
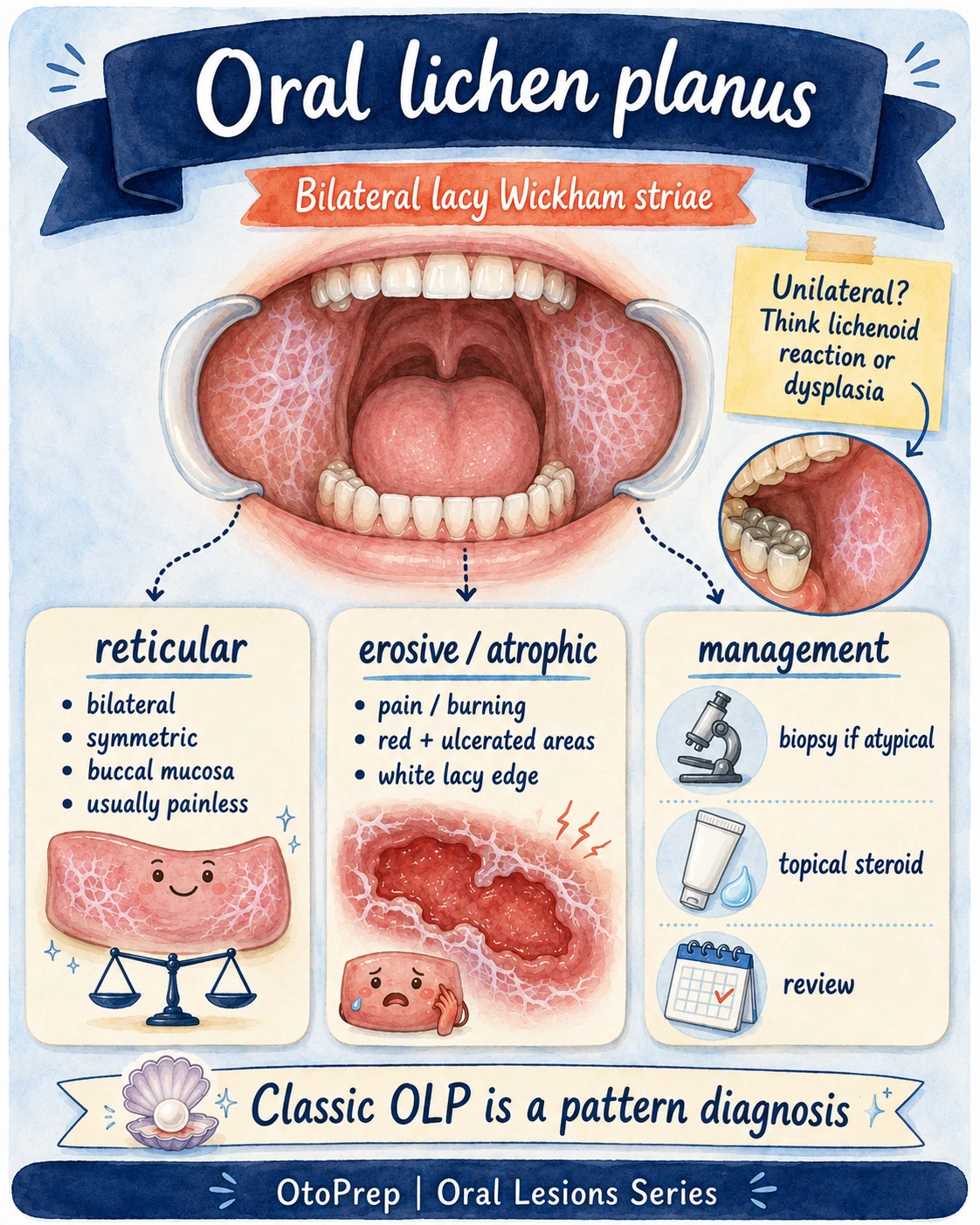
Oral lichen planus: bilateral lacy Wickham striae
Classic reticular oral lichen planus is a pattern diagnosis: bilateral, symmetric, lacy white lines, especially on the buccal mucosa.
| Pattern | Board clues | Management mindset |
|---|---|---|
| Reticular OLP | Bilateral, symmetric, lacy Wickham striae; commonly buccal mucosa; often painless. | Pattern diagnosis when classic; review and monitor. |
| Erosive / atrophic OLP | Burning, pain, erythema, ulcerated areas with a white lacy border. | Symptomatic disease is often treated with topical corticosteroid therapy under appropriate supervision. |
| Unilateral or atypical “OLP” | One-sided, irregular, isolated or changing lesion; may sit near dental restorations or look dysplastic. | Think lichenoid reaction, contact reaction, drug reaction or dysplasia; biopsy/referral threshold is lower. |
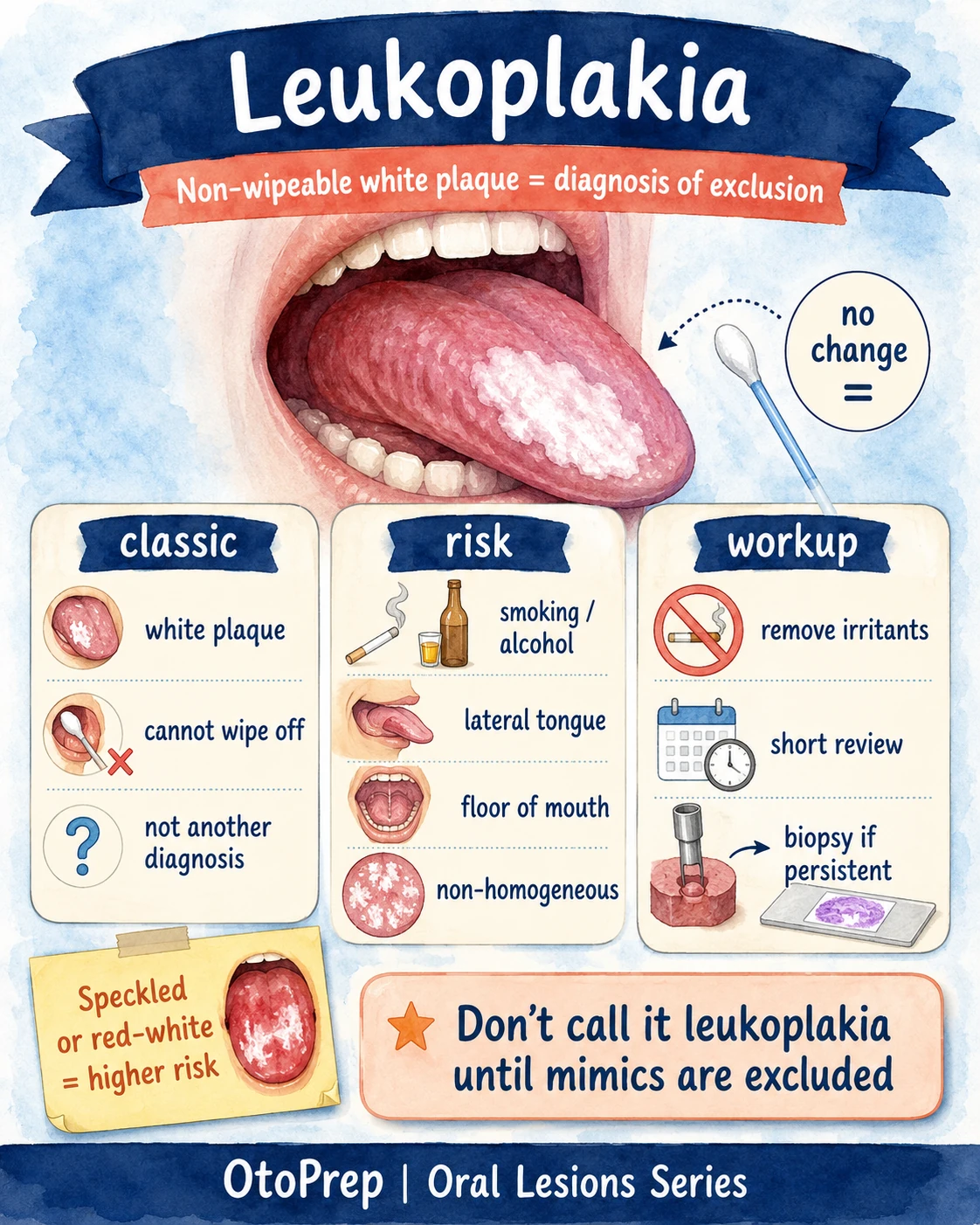
Leukoplakia: non-wipeable white plaque is a diagnosis of exclusion
Leukoplakia is not just “any white patch”. It is the pathway you enter after excluding other definable causes of a persistent white plaque.
- White plaque on oral mucosa.
- Cannot be wiped off.
- Not better explained by candidiasis, lichen planus, frictional keratosis, chemical burn, leukoedema or another diagnosis.
- Persistent after irritants are removed or after the presumed treatable cause has been treated.
Risk factors
- Smoking or smokeless tobacco
- Alcohol exposure
- Chronic irritation
- High-risk sites: tongue and floor of mouth
- Non-homogeneous or speckled morphology
Workup mindset
- Remove irritants
- Address candidal or traumatic mimics
- Arrange short-interval review
- Biopsy if persistent or suspicious
- Do not reassure without a diagnosis
Red flags: when a white oral lesion needs biopsy/referral mindset
The board-friendly phrase is: treat what is treatable, but biopsy or refer what is persistent, atypical or high risk.
| Finding | Why it matters | Board-ready next step |
|---|---|---|
| Unexplained oral ulceration lasting >3 weeks | Persistent ulceration is a cancer-referral red flag in many pathways. | Urgent assessment / suspected cancer pathway according to local guidance. |
| Red or red-white patch | Erythroplakia or erythroleukoplakia carries higher concern than a purely homogeneous white plaque. | Urgent dental/oral medicine/ENT assessment and biopsy consideration. |
| Induration, fixation, rolled border or mass | Suggests invasive or more aggressive pathology. | Biopsy/referral mindset. |
| Lateral tongue or floor-of-mouth lesion | Higher-risk oral cavity subsites for premalignant/malignant change. | Lower threshold for biopsy, especially if persistent or non-homogeneous. |
| Unilateral “lichen planus” | Classic reticular OLP is usually bilateral and symmetric. | Consider lichenoid reaction, trauma, dysplasia or malignancy; refer/biopsy if uncertain. |
| Persistence after appropriate antifungal treatment | A presumed candidal lesion should respond; non-response means the diagnosis may be wrong or incomplete. | Reassess risk factors, examine carefully and consider biopsy/referral. |
| Neck node, weight loss, dysphagia or systemic concern | Moves the question away from “benign oral lesion” and toward broader head-and-neck assessment. | Urgent specialist pathway. |
Common board traps: candidiasis vs leukoplakia vs lichen planus
The best exam answers show that you can avoid false reassurance and false certainty.
| Trap | Better answer |
|---|---|
| “It is white, so it is thrush.” | Only pseudomembranous candidiasis classically wipes off. Hyperplastic candidiasis can be non-wipeable and can mimic leukoplakia. |
| “It doesn’t wipe off, so it is leukoplakia.” | Non-wipeable means you must exclude mimics. Leukoplakia is a diagnosis of exclusion. |
| “Lichen planus is always harmless.” | Classic bilateral reticular OLP is a pattern diagnosis, but erosive, ulcerated, unilateral or changing lesions deserve caution and follow-up. |
| “Give antifungals and move on.” | Treat candidiasis, address risk factors and review the response. Persistence changes the plan. |
| “No pain means no problem.” | Many premalignant or malignant oral lesions may be painless early. |
See the original carousel
This article expands on the OtoPrep Instagram carousel covering white oral lesions, the wipe test, candidiasis, leukoplakia and oral lichen planus.
Practise this in exam format
Turn pattern recognition into marks with board-style stems, timed sets and analytics across head and neck, rhinology, otology, laryngology and paediatric ENT.
Also available: FRCS free trial · EBEORL-HNS free trial · ENT subscriptions
FAQ: white oral lesions
What is the first question to ask about a white oral lesion?
Ask whether it wipes off. A white plaque that wipes off suggests pseudomembranous candidiasis, especially if it leaves an erythematous base. A non-wipeable lesion needs further patterning and follow-up.
Does a non-wipeable white plaque always mean leukoplakia?
No. Non-wipeable lesions include leukoplakia, oral lichen planus, frictional keratosis, hyperplastic candidiasis and dysplasia or malignancy. Leukoplakia is a diagnosis of exclusion.
What is the classic pattern of oral lichen planus?
Classic reticular oral lichen planus is usually bilateral and symmetric, with lacy Wickham striae, often on the buccal mucosa. Unilateral or atypical lesions should prompt caution.
When should a white oral lesion be biopsied or referred?
Biopsy/referral should be considered for persistent lesions, uncertain diagnosis, red-white or speckled lesions, ulceration, induration, high-risk sites such as lateral tongue or floor of mouth, or failure to respond to appropriate treatment.
What is the board pearl for candidiasis vs leukoplakia?
Wipes off → candidiasis rises to the top. Persistent non-wipeable plaque → do not just reassure; exclude mimics and consider biopsy/referral if it persists or looks high risk.
Selected references and further reading
References are included to support medical accuracy and trust for a health-education page.
- NCBI Bookshelf: Oral Candidiasis — presentations, risk factors, wipeable pseudomembranous candidiasis and hyperplastic candidiasis.
- NCBI Bookshelf: Oral Leukoplakia — leukoplakia definition, diagnosis of exclusion, potentially malignant nature, risk factors and biopsy principles.
- NICE NG12: Suspected cancer recognition and referral — oral ulceration lasting more than 3 weeks and red/red-white oral patches.
- American Family Physician: Common Oral Lesions — oral lichen planus pattern recognition, Wickham striae and common oral lesion differentials.
- American Family Physician: Diagnosis and Treatment of Lichen Planus — biopsy in atypical cases and topical corticosteroids for mucosal erosive lesions.
- Google Search Central: Image SEO best practices — descriptive filenames, image placement, titles and alt text.
- Google Search Central: Article structured data — structured data for news, blog and article pages.
Keep learning
Useful next clicks for mocks, trials and structured ENT revision.
Educational content only. This page is designed for ENT examination preparation and should not be used as individual medical advice. Follow local guidelines and specialist input for real patients.


 High-Yield Deep-Dive • Rhinology
High-Yield Deep-Dive • Rhinology